Treatment of Mitral Valve Disease
Mitral Valve Stenosis
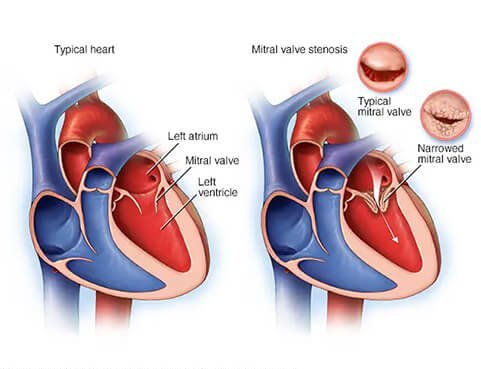
Mitral valve stenosis is a condition where the mitral valve, located between the left atrium and left ventricle of the heart, becomes narrowed and doesn’t open fully. This restricts blood flow into the heart’s main pumping chamber, making the heart work harder.
Symptoms may include breathlessness (especially during activity or when lying down), fatigue, swollen ankles, palpitations, dizziness, chest pain, or coughing up blood.
Treatment depends on severity. Mild cases may be managed with medications such as diuretics or anticoagulants. More severe cases may require procedures like balloon valvotomy, mitral valve repair, or replacement surgery.
What is mitral valve regurgitation?
The mitral valve is the valve between the left atrium and the left ventricle of your heart. In a normally functioning mitral valve, blood flows in a single direction from the left atrium to left ventricle. When your mitral valve's two leaflets do not close properly, blood flows back through the valve into the left atrium. This is called mitral regurgitation (or MR) and may also be referred to as a leaking heart valve. To compensate and keep blood flowing through the body, the left ventricle pumps harder. This strain can lead to other heart complications, which can be more serious if there is heart failure present.

Causes of mitral regurgitation
There are two types of mitral regurgitation, one type of mitral regurgitation is called primary MR (also called degenerative or organic). It is caused by a structural problem in the mitral valve itself. Primary MR can be related to either an individual or multiple components of the valve, such as leaflets, chordae or papillary muscles.
The other type is called secondary (or functional) mitral regurgitation. It is caused by heart disease that leads to an enlarged left ventricle and/or atrium, which prevents the valve from closing properly. This enlarging of the ventricle is most common in heart failure patients.
Symptoms
The signs and symptoms of mitral regurgitation depend on how advanced the insufficiency is and how quickly it has developed. Sometimes it causes few or no symptoms. However, if symptoms are present - especially in severe mitral regurgitation - they may include the following:
Shortness of breath, especially after exertion or when lying down
Drowsiness, brief unconsciousness, "blackness" before the eyes
Feeling of weakness and exhaustion, especially with increased activity (e.g. climbing stairs)
Irritable cough, which often worsens when lying down
Excessive water retention, swollen feet and ankles
Loss of appetite
Excessive urination at night
A leaky heart valve is tolerated by the body for a long time without those affected necessarily noticing. However, by the time symptoms occur, advanced heart valve disease is often already present. Severe mitral regurgitation is therefore a serious condition that must be diagnosed and treated in good time in order to prevent the consequences mentioned above.
What happens in the body if mitral regurgitation (MR) remains untreated
Untreated mitral regurgitation can lead to serious complications, including heart failure, irregular heart rhythm like atrial fibrillation, pulmonary hypertension, and potentially life-threatening cardiac arrhythmias. In severe cases, it can also increase the risk of blood clots, stroke, and endocarditis (infection of the heart lining and valve).
Diagnosis of mitral regurgitation
If mitral regurgitation is suspected, the doctor will listen to the heart with a stethoscope as one of the first diagnostic measures. The backflow of blood from the left ventricle through the diseased mitral valve into the left atrium of the heart can be clearly heard through the stethoscope.
There are also a number of other possibilities:
Echocardiography

One of the most important and informative examinations for detecting mitral regurgitation is an ultrasound examination of the heart, an echocardiogram. The doctor can see the blood flowing back from the left ventricle into the left atrium and the enlargement of the left atrium.
Echocardiography can be performed from the outside (transthoracic echocardiography) and also from the inside via the oesophagus (transoesophageal echocardiography). In a so-called stress echocardiography, the patient is exposed to a light load on the bicycle ergometer in order to accelerate the heartbeat, as it is difficult to assess the severity of the disease during an examination at rest. If this is not possible for health reasons, squeezing a foam ball several times quickly with the hand can also help to accelerate the heartbeat slightly and thus better visualise the mitral regurgitation.
Electrocardiogram examination (ECG)
An electrocardiogram (ECG) records the electrical activity of the heart and enables the detection of an abnormal heartbeat or damage to the heart muscle. An X-ray of the chest reveals an enlargement of the left atrium and water accumulation in the lungs (oedema). During a cardiac catheterisation, the amount of blood that flows back from the left ventricle through the diseased mitral valve into the left atrium with each heartbeat can be determined.
MitraClip™ therapy
The MitraClip™ Transcatheter Edge-to-Edge Repair System is a first-in-class TEER solution with proven performance and outcomes and is the only device that is cited in established guidelines for the treatment of MR. It includes an implant (clip) that is attached to the edges of your mitral valve to bring them together. The system has four clip sizes to allow your doctor to select the one that is right for your heart.



PATIENT STORY - Julie

Use of the MitraClip™
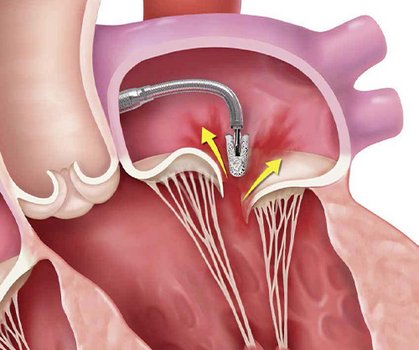
The procedure is performed under general anesthesia and the patient must stay in hospital for a few days afterwards. To access the mitral valve, a flexible, long guide catheter is inserted through a leg vein in the groin and advanced to the heart. This catheter is then used to attach the MitraClip™ to the mitral valve and ensure that it improves closure. During the procedure, doctors can check the position of the clip on the beating heart and, if necessary, correct it until the desired best possible reduction in insufficiency is achieved, as the reduction in mitral regurgitation is monitored in real time using a 3D ultrasound.You might need more than one clip implanted. This will be decided by your doctor and done during the same procedure.
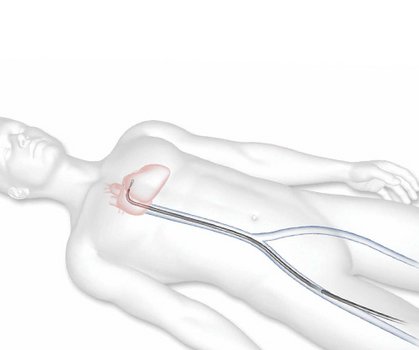
1. Your doctor will introduce the system through a vein in the groin area and will advance it to reach the heart.
2. The MitraClip implant will be guided from the right atrium to the left atrium and then ultimately to your mitral valve through the catheter.
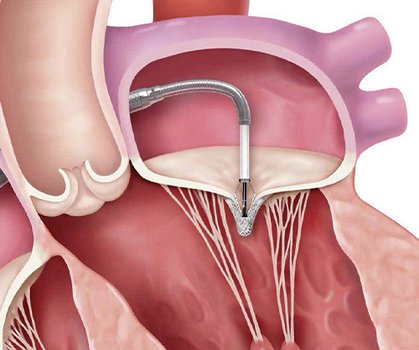
3. Your doctor will implant MitraClip at the appropriate position on your mitral valve. The MitraClip implant will grasp the mitral valve leaflets to bring their edges together and reduce mitral regurgitation.
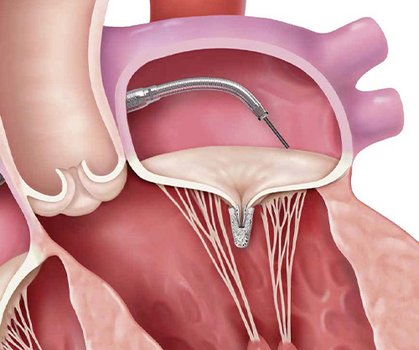
4. Once the implant is in place and working properly, the Clip Delivery System and the Steerable Guide Catheter will be removed from your body.
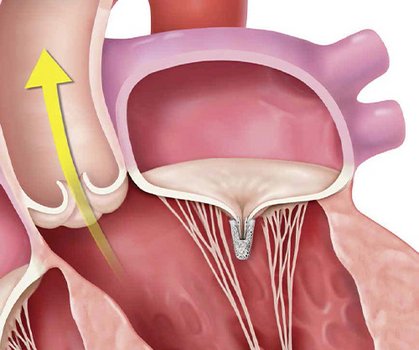
5. The MitraClip implant will become a permanent part of your heart, allowing your mitral valve to close more tightly and reduce the backward flow of blood.
Symptom Check
Who is the therapy suitable for?
Percutaneous mitral valve repair with a MitraClip™ is particularly suitable as an alternative for patients with severe mitral regurgitation who have a high surgical risk - for example, due to concomitant diseases or advanced age.1 For patients who suffer from symptoms of mitral regurgitation but are not candidates for open heart surgery, this minimally invasive procedure offers the chance to improve mitral regurgitation and its symptoms.2 This can lead to a significant improvement in quality of life3 for these patients.
There are numerous criteria that determine whether the MitraClip™ is a possible therapy for mitral regurgitation for each individual patient. Only a doctor can decide whether percutaneous mitral valve repair is an option for you or your loved one!
After the procedure

After percutaneous mitral valve repair with the MitraClip™, the patient initially remains in the intensive care unit for 24 hours and is then monitored in the normal hospital ward for three to five days. These are only guidelines - the treating physicians will adjust the length of stay according to individual needs and health requirements.
Most patients experience an improvement in clinical symptoms (improvement in breathlessness and exercise tolerance) immediately after the procedure.1 Nevertheless, medication must still be taken after percutaneous mitral valve repair, particularly to thin the blood and, if necessary, to treat any existing heart failure.2 It is very important that the doctor's instructions regarding medication that must be taken afterwards are followed in order not to jeopardise the patient's health.
After discharge from hospital, strenuous activities (such as lifting and carrying) should be avoided for at least 30 days. Most patients who have received a MitraClip™ do not need any special help at home beyond the current care required for all other conditions.3
The attending physician will therefore give you the patient ID card after the procedure, which you should then always carry with you.
Reports from patients who have received a MitraClip™
Over 300,000 patients* worldwide have already been treated with percutaneous mitral valve repair (m-TEER). In the following examples, they report on their disease, treatment with the MitraClip™ and their lives after the procedure.
Videos with patient reports

")
Patient Story - Luca

Patient Story - Scott
References
9-UK-5-16495-01 08-2025